Abstract
Sleep disturbances are a common symptom in individuals already diagnosed with Alzheimer’s disease (AD), but growing evidence indicates that sleep disruptions in midlife and older age could also represent one of the earliest signs of AD appearing decades before a formal diagnosis (Sabia et al., 2021). These sleep problems are not harmless. Trouble sleeping adds to harmful protein buildup, and Alzheimer’s makes sleep harder, together worsening memory (Winer et al., 2020). This paper reviews psychological approaches that address this cycle through two fields: cognitive psychology and neuropsychology. Cognitive Behavioral Therapy for Insomnia (CBT-I) is highlighted as the most effective cognitive psychology intervention while Gamma Entrainment Using Sensory Stimulation (GENUS) is highlighted as a promising intervention from the neuropsychological perspective. Together, these interventions offer a good strategy for improving sleep and potentially slowing the progression of AD. This review emphasizes the importance of early sleep interventions as a way to enhance quality of life for individuals with AD and their caregivers.
Keywords: Alzheimer’s disease, sleep disturbances, beta-amyloid, memory loss
Alzheimer’s Disease and Sleep Disturbances
Alzheimer’s disease (AD) is one of the most important public health challenges, and in 2025, an estimated 7.2 million adults aged 65 and older in the United States are living with AD (Alzheimer’s Association, 2025). This number is projected to significantly increase to 13.85 million people by 2060 (Rajan et al., 2021). The condition of AD is best known for memory loss, depression, anxiety, agitation, sleep difficulties, and challenges with daily activities like bathing or dressing (Ikeda et al., 2020). These symptoms affect not only patients but also place heavy emotional and financial burdens on families and caregivers (Huisman et al., 2025). By examining the two-way relationship between sleep and AD, tracing its progression across stages, and evaluating cognitive and neuropsychological interventions, this paper argues that Cognitive Behavioral Therapy for Insomnia (CBT-I) and Gamma Entrainment Using Sensory Stimulation (GENUS) offer the best evidence-based solutions for improving patient outcomes.
Although memory loss is the most familiar sign of AD, researchers are recognizing sleep problems as another critical early symptom (Winer et al, 2020). Studies show that persistent sleep of fewer than 6 hours in midlife raises the risk of dementia by about 30 percent, with AD being the most common form (Sabia et al., 2021). Poor quality deep sleep, especially reduced non-REM slow-wave sleep, weakens its protective role in memory consolidation and increases vulnerability to AD (Zavecz et al., 2023).
Disrupted sleep interferes with the brain’s ability to clear beta-amyloid and tau proteins, which are tied to AD (Ju et al., 2013). Brain scans show that getting less deep sleep and REM sleep is connected to damage in areas of the brain most at risk for AD (Cho et al., 2025). This connection suggests that ongoing sleep problems may gradually lead to lasting changes in brain structure (Cho et al., 2025).
Two-Way Relationship Between Sleep and AD
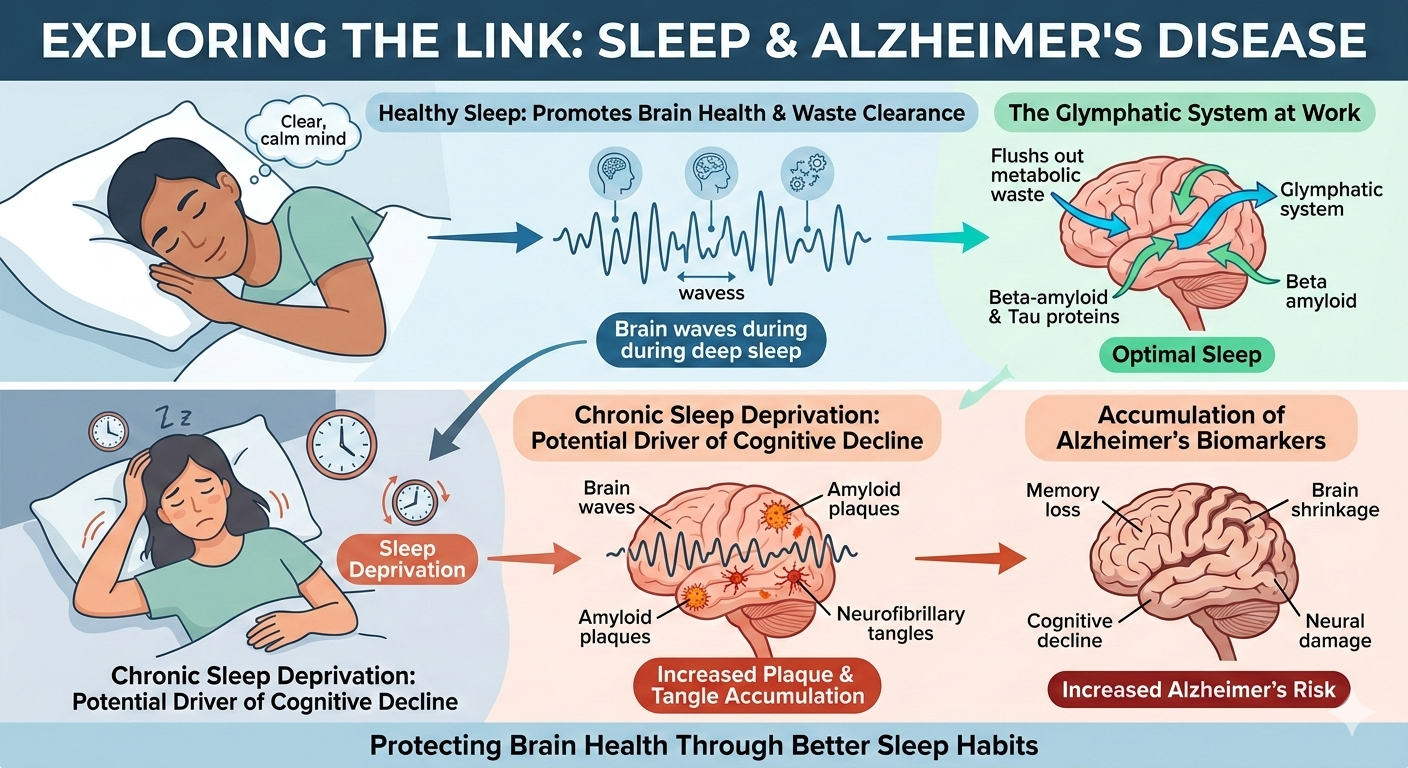
Sleep disruptions and AD are closely linked (Ju et al., 2023). Poor sleep can speed up the buildup of toxic proteins in the brain and accelerate cognitive decline, while early AD symptoms often make it harder to get quality rest (Ju et al., 2013). These proteins tend to accumulate in regions most affected by AD, such as the hippocampus and thalamus (Shokri-Kojori et al., 2018). One reason for this accumulation is that disrupted sleep interferes with glymphatic clearance (Xie et al., 2013). This is the brain’s natural process for flushing out waste during slow-wave sleep (Xie et al., 2013). When this system breaks down, protein deposits grow and damage vulnerable brain areas (Pathmanathan et al., 2025). This breakdown in sleep appears to have serious consequences. In one study, it was found that older men over 70 who struggled to fall asleep or stay asleep were found to have a 192% higher risk of developing AD (Benedict et al, 2014). These results are alarming.
Progression Across AD Stages
This cycle of poor sleep becomes more pronounced over time (Volicer et al., 2001). In the early to middle stages of AD, patients often face frequent nighttime awakenings, shorter periods of deep sleep, excessive daytime sleepiness, and sundowning behaviors such as evening agitation (Volicer et al., 2001). As the disease progresses, sleep disruptions intensify and Alzheimer’s patients spend longer hours asleep during the day and experience interrupted sleep at night (Huisman et al., 2025). Caregivers sometimes describe this phase as living on a flipped schedule because it affects their sleep and daytime activities as well (Huisman et al., 2025). This breakdown in sleep not only accelerates cognitive decline but also contributes to emotional and behavioral difficulties (Huisman et al., 2025). This further complicates care in the later stages of AD (Huisman et al., 2025).
Cognitive Psychology to the Rescue
Cognitive psychology looks at what’s happening inside the mind and shows how skills like paying attention and problem-solving affect daily living (Jouve, 2025). These same mental processes also play a role in sleep and AD (Winer et al., 2020). Many people with memory problems struggle with nighttime confusion and anxiety at bedtime (Li & Yu, 2024). This is something many caregivers mention as it becomes a fear of the night rather than just difficulty sleeping (Li & Yu, 2024). These thoughts can worsen insomnia and daytime fatigue. Cognitive interventions can help break this cycle by challenging unhelpful beliefs and reducing anxiety at night (Li & Yu, 2024). Overall, cognitive psychology offers two helpful interventions that are relevant to sleep and AD. The first is cognitive training (Diamond et al., 2015) and the second is Cognitive Behavioral Therapy for Insomnia, or CBT-I (Li & Yu, 2024).
Intervention 1: Cognitive Training
The Healthy Brain Ageing Cognitive Training (HBA-CT) program, developed in the Diamond study, combines computerized tasks with psychoeducation to strengthen mental skills such as memory and attention (Diamond et al., 2025). In AD, early declines in both often disrupt daily structure and can also throw off sleep patterns at night (Cho et al., 2025). HBA-CT offers a way to rebuild some of that structure (Diamond et al., 2015).
The psychoeducation sessions were 1 hour each and delivered weekly in small groups by a specialist using PowerPoint presentations (Diamond et al., 2015). These sessions covered stress reduction, managing depression and anxiety, sleep hygiene, the role of physical exercise, information on diet and nutrition, and practical sessions for remembering appointments and using cues (Diamond et al., 2015). The computerized cognitive exercises were twice weekly and involved word-list learning, story recall exercises, digit span exercises, problem solving and puzzles, and trail making test activities (Diamond et al., 2015).
The results were eye-opening. Compared to controls, participants in the cognitive training group showed major improvements in sleep (Diamond et al., 2015). They also showed better memory performance and reduced symptoms of depression (Diamond et al., 2015). This connection between better memory, mood, and sleep makes sense because once people feel more in control of their thinking, their nights often become less chaotic (Diamond et al., 2015).
Intervention 2: Cognitive Behavioral Therapy for Insomnia (CBT-I)
CBT-I is a structured therapy that helps people change the thoughts and habits that keep insomnia going (Li & Yu, 2024). It teaches skills like limiting time spent awake in bed, sticking to regular sleep schedules, and challenging worries about not sleeping (Li & Yu, 2024). In simple terms, CBT-I helps retrain the brain to associate the bed with sleep, not frustration. CBT-I also helps to reduce the nighttime anxiety that often makes falling asleep harder (Li & Yu, 2024). Many people describe CBT-I as learning how to sleep because it directly targets both the mental and behavioral patterns that disrupt sleep (Li & Yu, 2024).
The core idea behind CBT-I is that beliefs, expectations, and routines surrounding sleep can either support healthy sleep or get in the way of it (Li & Yu, 2024). Common problems include worrying about not sleeping, thinking normal nighttime sensations as something concerning, spending too much time in bed awake, and keeping irregular sleep and wake times (Li & Yu, 2024). These problems can become even more noticeable as cognitive decline begins and anxiety, confusion, and disrupted routines make sleep problems more likely (Winer et al., 2020). CBT-I improves sleep by helping people change the thoughts and habits that keep them awake at night (Li & Yu, 2024).
Argument for Chosen Cognitive Psychology Intervention: CBT-I
Among the available interventions from cognitive psychology, Cognitive Behavioral Therapy for Insomnia (CBT-I) has shown the strongest benefits for people with mild cognitive impairment, a group at risk for AD (Li & Yu, 2024). It helps people change habits and thoughts that make it harder to sleep so they can rest better and think more clearly (Li & Yu, 2024). Instead of working around the issue, CBT-I directly reshapes the patterns that keep insomnia going (McCrae et al., 2023). This is especially important in AD because sleep disturbances can create a harmful cycle (Spira & Gottesman, 2017). Improving sleep quality with CBT-I may help slow or interrupt the cycle of insomnia and cognitive decline (Li & Yu, 2024).
The research is also a compelling part as CBT-I remains effective even for people experiencing early mild cognitive impairment (Li & Yu, 2024). Participants with mild cognitive impairment experienced significant improvements in sleep after completing CBT-I therapy (Li & Yu, 2024). They also reported feeling less anxious about sleep (Li & Yu, 2024). That matters because for many people, the anxiety about not sleeping becomes as disruptive as the insomnia itself. Breaking this cycle often brings a huge sense of relief for both the person suffering with AD and the caregivers. CBT-I has also shown promise for caregivers (McCrae et al., 2023). An ongoing pilot study that ends in 2027 shows that a web-based CBT-I program is effective in improving sleep and reducing insomnia symptoms in dementia caregivers (McCrae et al., 2023).
Overall, CBT-I seems to promote the kind of sleep that actually protects the brain. Strategies like sleep restriction and control can help increase the deep sleep linked to memory consolidation (Li & Yu, 2024). Taken together, these findings show why CBT-I is the strongest cognitive psychology intervention. It directly addresses the thinking patterns and habits that disrupt sleep and is supported by research.
Neuropsychology Approaches
Neuropsychology looks at how the brain affects the way we think and behave. This field is important for understanding AD because it shows how problems in brain circuits that control sleep, memory, and sensory processing, make symptoms of AD worse over time (Ikeda et al., 2020). In other words, neuropsychology gives us a roadmap of which brain areas are falling behind and helps us figure out where to intervene. Two promising examples are tailored lighting interventions (Figueiro et al., 2019) and Gamma Entrainment Using Sensory Stimulation, or GENUS (Chan et al., 2022). Both interventions show that by guiding the brain’s natural rhythms, people with AD can have improved sleep and function better during the day (Figueiro et al., 2019; Chan et al., 2022).
Intervention 1: Tailored Lighting Intervention
Tailored lighting interventions use blue light to stimulate the circadian system (Figueiro et al., 2019). This matters because sleep problems in AD are closely tied to disruptions in the brain’s circadian rhythm (Volicer et al., 2001). This is the internal clock that helps regulate when we feel awake and when we feel sleepy (Volicer et al., 2001). As AD progresses, the brain becomes less sensitive to everyday light cues so regular daylight alone often isn’t enough to keep the body’s internal clock in sync (Volicer et al., 2001). It’s similar to traffic lights on a busy street being out of sequence. Drivers are confused and everything becomes chaotic. Tailored lighting addresses this issue by providing structured exposure to bright blue light during the day (Figueiro et al., 2019). In a randomized clinical trial, this type of lighting significantly improved sleep quality, reduced depression scores, and lowered agitation (Figueiro et al., 2019).
This approach works by using lamps and light boxes that are designed to emit specific wavelengths and intensities (Figueiro et al., 2019). The lights are strong enough to suppress melatonin and wake up the circadian system (Figueiro et al., 2019). Overall, this stimulates specialized retinal cells that communicate directly with the brain’s master clock (Figueiro et al., 2019). Basically, it reminds the brain what time of day it is. It’s like sending the brain a daytime signal. These signals help recalibrate the internal clock so that it better matches the natural day and night cycle (Figueiro et al., 2019). When this alignment improves, sleep tends to become more stable, and people experience better rest and mood stability (Figueiro et al., 2019).
Intervention 2: Gamma Entrainment Using Sensory Stimulation (GENUS)
Gamma Entrainment Using Sensory Stimulation (GENUS) uses rhythmic sensory stimulation to help brain activity patterns (Chan et al., 2022). It uses flickering light and sound, both pulsing at 40 Hz (Chan et al., 2022). This frequency is linked to healthy brain activity (Iaccarino et al., 2016). Foundational work in mice showed that 40 Hz light flicker reduced amyloid-beta (Iaccarino et al., 2016). This paved the way for human studies (Iaccarino et al., 2022). What GENUS does is it tries to nudge the brain back into a healthier rhythm by using light and sound to help the brain to naturally follow this 40 Hz pattern (Chan et al., 2022).
Specifically, GENUS works by boosting gamma activity, which are the brain’s fastest electrical rhythms (Chan et al., 2022). These rhythms act like a steady beat that helps different regions of the brain stay in sync and share information (Chan et al., 2022). When gamma activity is strengthened, the brain’s communication becomes more coordinated (Chan et al., 2022).
Research so far suggests that GENUS is safe, well-tolerated, and may benefit both sleep and cognitive functioning (Chan et al., 2022). In one study after 3 months of daily sessions, adults with mild AD who received daily 40 Hz stimulation showed less hippocampal atrophy, better memory, and improved sleep patterns (Chan et al., 2022). Many participants also seemed more alert and engaged during the day (Chan et al., 2022).
Argument for Chosen Neuropsychology Intervention: GENUS
Among the neuropsychology interventions reviewed, GENUS emerges as the most promising option for improving both brain function and sleep in people with AD. GENUS uses synchronized light and sound pulsed at 40 Hz to stimulate gamma activity (Chan et al., 2022). Research shows that this type of stimulation can reduce amyloid accumulation, strengthen gamma fluctuations, and support attention and cognitive performance even in people with mild AD (Chan et al., 2022). In animal models, daily 40 Hz stimulation also enhanced microglial activity suggesting that gamma entrainment may trigger protective immune responses in the brain (Iaccarino et al., 2016). Regular 40 Hz stimulation may give people with early cognitive decline a noticeable boost in sleep quality and everyday functioning (Chan et al., 2022). It’s like giving the brain a gentle nudge to get its timing and communication back in sync. For many families, even small gains can make daily life feel more hopeful.
What sets GENUS apart is how it directly interacts with the neural circuits affected by the disease (Chan et al., 2022). While other interventions may focus on changing behavior or modifying the environment, GENUS aims to influence the underlying biology (Chan et al., 2022). It targets the brain mechanisms that contribute to cognitive decline and disrupted sleep (Chan et al., 2022). This is the biggest advantage of GENUS is that it may actually influence the course of AD and improve processes linked to Alzheimer’s progression (Chan et al., 2022).
When combined with its ease of use and growing clinical support, GENUS becomes a compelling choice. It provides a promising, research supported way to help improve sleep, strengthen thinking skills, and possibly slow the changes that make Alzheimer’s worse over time (Chan et al., 2022). While GENUS is still an emerging intervention and more research is needed, early studies seem encouraging.
Conclusion
Sleep disturbances and AD reinforce one another in ways that accelerate cognitive decline. However, this relationship also creates an opportunity. Sleep is one of the few factors that can be strengthened early. Looking at CBT-I and GENUS together shows that each one helps in a different but complementary way. CBT-I gives people the tools and routines they need to sleep more consistently at night while GENUS works on the brain’s timing signals. When used together, these approaches reinforce each other. Better habits make the brain more responsive to healthy rhythms and healthier rhythms make it easier to stick with good sleep routines.
Looking ahead, combining cognitive and neuropsychological interventions could become a standard part of early Alzheimer’s treatment. It’s not a cure, but it’s a way to give people more good days. More research is needed to understand the best timing and long-term effects of GENUS and to determine how CBT-I can be adapted for people with increasing cognitive challenges. The evidence so far suggests that sleep is a factor that can shape the course of the disease.
This combined approach of CBT-I and GENUS interventions can help daily functioning and reduce the nighttime confusion that often burdens families. Caregivers benefit as well since improved sleep means calmer nights and less stress. Even small gains can make daily life more hopeful for people living with Alzheimer’s and for the people who care for them. Better sleep may not stop Alzheimer’s, but it can help people stay independent longer and feel more like themselves. In the end, improving sleep is one of the simplest and most helpful tools we have for supporting people living with Alzheimer’s disease. It’s an achievable step toward preserving dignity, independence, and well-being in the face of a devastating disease.
References
Alzheimer’s Association. (2025). 2025 Alzheimer’s disease facts and figures. Alzheimer’s & Dementia, 21(4). https://doi.org/10.1002/alz.70235
Benedict, C., Byberg, L., Cedernaes, J., Hogenkamp, P. S., Giedratis, V., Kilander, L., Lind, L., Lannfelt, L., & Schiöth, H. B. (2014). Self-reported sleep disturbance is associated with Alzheimer’s disease risk in men. Alzheimer’s & Dementia, 11(9), 1090–1097. https://doi.org/10.1016/j.jalz.2014.08.104
Chan, D., Suk, H.-J., Jackson, B. L., Milman, N. P., Stark, D., Klerman, E. B., Kitchener, E., Fernandez Avalos, V. S., de Weck, G., Banerjee, A., Beach, S. D., Blanchard, J., Stearns, C., Boes, A. D., Uitermarkt, B., Gander, P., Howard, M., Sternberg, E. J., Nieto-Castanon, A., & Anteraper, S. (2022). Gamma frequency sensory stimulation in mild probable Alzheimer’s dementia patients: Results of feasibility and pilot studies. PLOS ONE, 17(12), e0278412. https://doi.org/10.1371/journal.pone.0278412
Cho, G., Mecca, A. P., Buxton, O. M., Liu, X., & Miner, B. (2025). Lower slow wave sleep and rapid eye movement sleep are associated with brain atrophy of AD-vulnerable regions. Journal of Clinical Sleep Medicine, 21(7). https://doi.org/10.5664/jcsm.11630
Diamond, K., Mowszowski, L., Cockayne, N., Norrie, L., Paradise, M., Hermens, D. F., Lewis, S. J., Hickie, I. B., & Naismith, S. L. (2015). Randomized controlled trial of a healthy brain ageing cognitive training program: effects on memory, mood, and sleep. Journal of Alzheimer’s disease: JAD, 44(4), 1181–1191. https://doi.org/10.3233/JAD-142061
Figueiro, M. G., Plitnick, B., Roohan, C., Sahin, L., Kalsher, M., & Rea, M. S. (2019). Effects of a Tailored Lighting Intervention on Sleep Quality, Rest–Activity, Mood, and Behavior in Older Adults with Alzheimer Disease and Related Dementias: A Randomized Clinical Trial. Journal of Clinical Sleep Medicine, 15(12), 1757–1767. https://doi.org/10.5664/jcsm.8078
Huisman, C. A. M., Huisman, E. R. C. M., Brankaert, R. G. A., & Kort, H. S. M. (2025). Sleep at home for older persons with dementia and their caregivers: a qualitative study of their experiences and challenges. European Journal of Ageing, 22(1), 28. https://doi.org/10.1007/s10433-025-00858-w
Iaccarino, H. F., Singer, A. C., Martorell, A. J., Rudenko, A., Gao, F., Gillingham, T. Z., Mathys, H., Seo, J., Kritskiy, O., Abdurrob, F., Adaikkan, C., Canter, R. G., Rueda, R., Brown, E. N., Boyden, E. S., & Tsai, L.-H. (2016). Gamma frequency entrainment attenuates amyloid load and modifies microglia. Nature, 540(7632), 230–235. https://doi.org/10.1038/nature20587
Ikeda, Y., Han, G., Maruta, M., Hotta, M., Ueno, E., & Tabira, T. (2020). Association between Daily Activities and Behavioral and Psychological Symptoms of Dementia in Community-Dwelling Older Adults with Memory Complaints by Their Families. International Journal of Environmental Research and Public Health, 17(18), 6831. https://doi.org/10.3390/ijerph17186831
Jouve, X. (2025). Ethics & Appropriate Use. Cogn-IQ. https://www.cogn-iq.org/learn/theory/cognitive-psychology/
Ju, Y.-E. S., Lucey, B. P., & Holtzman, D. M. (2013). Sleep and Alzheimer disease pathology—a bidirectional relationship. Nature Reviews Neurology, 10(2), 115–119. https://www.nature.com/articles/nrneurol.2013.269
Li, P. W. C., & Yu, D. S. F. (2024). Empowerment‐based cognitive behavioral therapy for insomnia in persons with mild cognitive impairment: A sequential explanatory mixed‐method pilot study. Journal of Sleep Research, 33(5). https://doi.org/10.1111/jsr.14131
McCrae, C. S., Curtis, A. F., Stearns, M. A., Nair, N., Golzy, M., Shenker, J. I., Beversdorf, D. Q., Cottle, A., & Rowe, M. A. (2023). Development and Initial Evaluation of Web-Based Cognitive Behavioral Therapy for Insomnia in Rural Family Caregivers of People with Dementia (NiteCAPP): Mixed Methods Study. JMIR aging, 6, e45859. https://doi.org/10.2196/45859
Pathmanathan, J., Westover, M. B., Sudhir Sivakumaran, Donoghue, J., & Puryear, C. B. (2025). The role of sleep in Alzheimer’s disease: a mini review. Frontiers in Neuroscience, 19(1428733). https://www.frontiersin.org/journals/neuroscience/articles/10.3389/fnins.2025.1428733
Rajan, K. B., Weuve, J., Barnes, L. L., McAninch, E. A., Wilson, R. S., & Evans, D. A. (2021). Population estimate of people with clinical Alzheimer’s disease and mild cognitive impairment in the United States (2020-2060). Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association, 17(12), 1966–1975. https://doi.org/10.1002/alz.12362
Sabia, S., Fayosse, A., Dumurgier, J., van Hees, V. T., Paquet, C., Sommerlad, A., Kivimäki, M., Dugravot, A., & Singh-Manoux, A. (2021). Association of sleep duration in middle and old age with incidence of dementia. Nature Communications, 12(1), 2289. https://doi.org/10.1038/s41467-021-22354-2
Shokri-Kojori, E., Wang, G.-J., Wiers, C. E., Demiral, S. B., Guo, M., Kim, S. W., Lindgren, E., Ramirez, V., Zehra, A., Freeman, C., Miller, G., Manza, P., Srivastava, T., De Santi, S., Tomasi, D., Benveniste, H., & Volkow, N. D. (2018). β-Amyloid accumulation in the human brain after one night of sleep deprivation. Proceedings of the National Academy of Sciences, 115(17), 4483–4488. https://doi.org/10.1073/pnas.1721694115
Spira, A. P., & Gottesman, R. F. (2017). Sleep disturbance: an emerging opportunity for Alzheimer’s disease prevention? International Psychogeriatrics, 29(4), 529–531. https://www.intpsychogeriatrics.org/article/S1041-6102(24)00998-0/fulltext
Volicer, L., Harper, D. G., Manning, B. C., Goldstein, R., & Satlin, A. (2001). Sundowning and Circadian Rhythms in Alzheimer’s Disease. American Journal of Psychiatry, 158(5), 704–711. https://doi.org/10.1176/appi.ajp.158.5.704
Winer, J. R., Mander, B. A., Kumar, S., Reed, M., Baker, S. L., Jagust, W. J., & Walker, M. P. (2020). Sleep Disturbance Forecasts β-Amyloid Accumulation across Subsequent Years. Current Biology, 30(21), 4291-4298.e3. https://doi.org/10.1016/j.cub.2020.08.017
Xie, L., Kang, H., Xu, Q., Chen, M. J., Liao, Y., Thiyagarajan, M., O’Donnell, J., Christensen, D. J., Nicholson, C., Iliff, J. J., Takano, T., Deane, R., & Nedergaard, M. (2013). Sleep Drives Metabolite Clearance from the Adult Brain. Science, 342(6156), 373–377. https://pmc.ncbi.nlm.nih.gov/articles/PMC3880190/
Zavecz, Z., Shah, V. D., Murillo, O. G., Vallat, R., Mander, B. A., Winer, J. R., Jagust, W. J., & Walker, M. P. (2023). NREM sleep as a novel protective cognitive reserve factor in the face of Alzheimer’s disease pathology. BMC Medicine, 21(1). https://doi.org/10.1186/s12916-023-02811-z